Breast Lift & Augmentation
Breast LIFT & Augmentation
Breast Lift & Augmentation Surgery from Dr. Moulton Barrett
Breast lift surgery is designed to improve the appearance of sagging or ptotic breasts. The Breast Lift and augmentation
To find out if a breast lift and augmentation is right for you, request a consultation with Dr. Moulton-Barrett.
The etiology is varied and can be due to several components but gravity seems to be a common factor. Younger patients are more prone to ptosis if breast size is excessive or if the skin is thin. Ptosis in middle-aged patients usually is due to postpartum changes; the breast skin is stretched during lactation or engorgement, and afterward the breast gland atrophies, leaving loosened skin. Finally, in postmenopausal patients, further atrophy, gravity, loss of skin elasticity due to age, and weight gain are factors in creating breast ptosis.
In most instances, breast mastopexy has no true medical indication and is performed primarily for aesthetic reasons. The main exception to this is in postmastectomy
While descriptions of reduction mammoplasty were reported as early as Paulus of Aegina (625-690 AD), not until the late 19th century was emphasis placed on correcting ptosis of the breast. Much of the history of mastopexy parallels breast reduction, both attempt to alter the shape of the breast and skin
Wise (1956) defined the preoperative geometric marking system most commonly used today. Gonzalez-Ulloa (1960) first advocated mastopexy with augmentation for ptosis with hypoplasia or atrophy. Benelli (1990) reported the use of the periareolar round block or purse string mammoplasty. Hall-Findley (1999) used a
Mastopexy presents one of the greatest challenges to the breast surgeon but previous techniques have drawbacks. Although breast implants may provide the upper pole projection patients often desire, they present specific risks and complications.
Mastopexy Augmentation: Superior Crescent
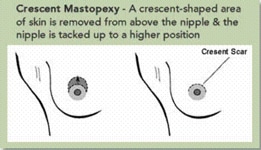
For patients with mild sagging, excess breast skin in the upper half of the breast, requesting no more than 2cm of nipple/areola lift and a normal amount of skin in the lower half, a semi-circular incision is made on the upper border of the areola. A

Mastopexy Augmentation: Anchor Incision
The balance between opposing forces of removal of excess and ptotic breast skin and the addition of breast volume is a careful one. The ultimate goal is to design the breast with sufficient skin tension to fight the tendency of recurrent ptosis and laxity without

Breast Implant Warranty
The latest warranty information is an increasingly complicated subject. The variables include saline versus silicone, rupture versus capsular contracture, year of implantation and may be quite specific to the actual implant company. To understand what warranty exists for a particular implant, please click for more detailed implant warranty information.
Frequently Asked Questions
To find out more about arm lifts and other body contouring procedures, request a consultation with Dr. Moulton-Barrett at one of his Bay Area offices. Board-certified plastic surgeon Rex Moulton-Barrett, M.D., offers advanced care and procedures for Bay Area residents. He has offices in Alameda and Brentwood, CA.
BREAST PROCEDURES
Our Clinics
Alameda Clinic
2070 Clinton Ave
Fourth Floor
Alameda, CA 94501
Phone (510) 864-1800
Brentwood Clinic
1280 Central Blvd
Suite J-5
Brentwood, CA 94513
Phone (925) 240-8775
ALAMEDA OFFICE
BRENTWOOD OFFICE
Alameda Location
2070 Clinton Ave, Alameda, CA 94501
510-864-1800
Brentwood Location